
The following is a transcript of an interview with Professor Johan Giesecke, M.Sc., M.D., Ph.D., the State Epidemiologist from 1995 to 2005 and the leading consultant on the so-called Swedish model — so-called, I say, because it is in my opinion a horribly sad testament to the indoctrination that’s taken place in one-month’s time: indoctrination which has made inconceivable, for many millions, the true idea that voluntary action among free humans is far more effective than authoritarian control and force.
The transcript is not boring at all, nor overly technical, and I urge readers to read it through. It is a levelheaded analysis, and it gives a great deal of real insight. It also vindicates what many have said from the beginning — and his last statements are sure to shock and outrage many millions among the masses who have not chosen to undertake the task of sifting through the data themselves, weighing it in the totality of context, but rather chose the method of dogmatism and blind-or-purblind belief. Please take special note also of how the initial goal of forced social distancing — easing or slowing the burden on hospitals — has completely shifted, as many warned, to an indefinite lockdown: a total and unequivocal violation of rights, both person and property, and the danger from which cannot be overstated. If any of you have any doubt at all that power once gotten cannot easily be torn away from power-holders, your doubts will shortly be dispelled.
But first this news, which is bad — very bad — yet will be made even worse if government institutes policies aimed at “stabilization,” which means price controls, which in turn create greater shortages:

Professor Johan Giesecke worked as infectious disease clinical doctor working with AIDS patients during the 1980s and trained at the London School of Tropical Medicine in the 1990s before returning to Sweden. Since then he has been chief scientist at the European Center for Disease Control, provided advice to the World Health Organization’s Director-General, and continues to serve as a consultant advisor to Anders Tegnell at the Swedish Agency for Public Health.
Dr. Giesecke speaks out against draconic measures, which so far are not evidence-based, elaborating on how the Swedes have done things differently and how they could have done even better.
Q: There’s been a lot of confused thinking and a lot of confusion about what the correct response to a threat such as COVID-19 and should be – and I just wanted to begin by getting your, kind of summary, thoughts of – of you know, how Sweden is differing from other countries and why you think that is.
A: The main reason is that we, or the Swedish government, decided early in January that the measures we should take against the pandemic should be evidence-based. And when you start looking around for the measures that are being taken now by different countries you find that very few of them have the shred of evidence base. But one we know, that’s known for a hundred and fifty years or more, and that is washing your hands is good for you and good for others when you’re in an epidemic. But the rest – like border closures, school closures, social distancing – there’s almost no science behind most of these.
Q: So what is the current policy in Sweden? Social distancing is part of the policy, isn’t it? What is the regime that Sweden has gone with?
A: The main difference to other countries is that there is no – you’re not locked up in your home. If you go out to buy food, or groceries, or drugs – I mean medicines – there’s no police to stop you in the street and ask you what you’re doing here. That’s one thing. People are asked to stay inside, but there is no reinforcement or enforcement of that. People do it anyway. So that’s one. We have the rule that the crowd cannot be bigger than 50 people.
Q: So I can still have an event for 49 people? (Although I won’t.)
A: Yes, you could. The schools – the upper schools are closed; secondary education and universities closed; schools up to age 15, 16 schools are open. What more do we have? Don’t – the nursing homes, or houses for old people, are closed to visitors.
Q: So it sounds like it’s a moderate social distancing regime then, at the moment?
A: Yes, it is. Sorry it’s very similar to the one that the UK had before there was a famous paper in – by – the Imperial College, by the modelers who made models for infectious diseases that came out on the day after you made a u-turn in England.
Q: Yes, tell us the original strategy in the UK and became known as a kind of herd immunity strategy, that’s what it was called. Before we get on to talk about the Imperial model – which I would like to talk about – is it correct to call it herd immunity and, and is that the Swedish strategy?
A: It’s not a strategy, but it’s a by-product of the strategy. But the strategy is to protect the old and the frail; try to minimize their risk of becoming infected, and taking care of them if they get infected. If you do that – the way we’re doing it – you would probably get herd immunity and then – but that’s a byproduct order, it’s not the main reason to do it.
Q: So you were saying and so the initial UK response seemed to be similar to what you – Sweden – is doing now, and you thought that was better?
A: Yeah. No, I think it is very good actually, and we were very pleased we were having the same policies as the UK: that gave some credibility to what we were doing. But then Mr. Johnson made his hundred and eighty degree turn.
Q: Yes, so there might have been a lot of other political factors involved. He was definitely under a lot of pressure, because lots of European countries were doing a formal lockdown at that point, but the turning point did seem to be that Imperial College report which forecast 510,000 deaths in the UK with a completely unmitigated approach 250,000 deaths with a mitigated approach – which is roughly equivalent to what you’re doing in Sweden – and then it suggests that he might be as few as 20,000 if we did a full suppression or lockdown. What was your impression of that paper?
A: I think it’s not very good. And the thing that they miss little is, any models for infectious disease spread are very popular – many people do them, they’re good for teaching – they seldom tell you the truth because, I make a small parenthesis, which model could have assumed that the outbreak would start in northern Italy in Europe? Difficult to model that one. And any such model – it looks complicated, there are strange mathematical formulas and integrals signs and stuff – but it rests on the assumptions, and the assumptions in that ought to be heavily criticized for – I won’t go through that it; would take to the rest of your day if I went through them all. The paper was never published – scientifically – it’s not peer-reviewed, which scientific paper should be. It’s just an internal departmental report from Imperial, and it’s fascinating, I don’t think any other scientific endeavor has made such an impression on the world as that, rather debatable, paper.
Q: So it’s your impression that it was overly pessimistic?
A: Yes – oh yes, very much so.
Q: So what you know I mean I guess it comes down to some degree of speculation but, what’s your impression of how serious the disease is and what kind of fatalities we would be looking at if we had a more moderate or more mitigated approach?
A: What’s the number of deaths in the UK now? I don’t know. [13 thousand.] So you’re getting close to 20 now. [Yeah.] But probably not 510,000. I think – well let me go back one step. One thing that the model has missed is that it assumes that a hospital capacity will remain the same, and that’s not what’s happening anywhere. I mean in Sweden we tripled our intensive care capacity, and I think there’s happening in the UK as well, but the paper completely overlooks that. It’s, as I said it’s such a static thing.
Q: Hmm. So just to sort of to come back on this, we had the argument, what people watching will be asking – and I think what most people who support the lockdown would say, and that is the overwhelming majority of people in politics and in the media – is that the reason the curve is now flattening, and the numbers of deaths are gradually coming down on a daily basis, is because of the lockdown and that it shows that the policy has worked. And Professor Neil Ferguson who wrote the, or led the Imperial papers, suggests that he stands by his prediction that 500,000 people would have died had that not taken place. So if it wasn’t the lockdown that has been flattening our curve what else could it have been?
A: One thing is immunity; the other is that the people who are frail and old will die first. And when that group of people is sort of thinned out, you will get less deaths as well. The other thing is that when you start your exit strategy – that’s the favorite word now in all this public effort: the exit strategy – when you start that one you’ll have some other deaths that we had already.
Q: Yes so, I mean, does that mean then that, as the disease passes through the population, you know, are we gonna see second and third spikes now after this?
A: It would be part of the exit strategy, because the only way to check that your, if you’re taking away one restriction and – say we open the schools again as an example – how do you evaluate that? You have to see numbers are going up again; more people are dying. We have to stop that. We have to pull back that softening and try another. That’s what exit strategy will be in all countries. Countries will ease up a little on a restriction; see what happens over the next 2-3 weeks. “Oooh, it didn’t work very well, we’d assumed that.” We try another restriction. Well if that one – “Oh, it worked!” And that so this is every country will have to do it that way. And that means that the increasing number of deaths will be part of checking which strategy should be kept and not…
Q: So what should we be doing instead?
A: Well you can’t. When I first heard, which is now six week ago, about the different draconic measures that were taken I asked myself: How are they going to climb down from that one? When will they open the schools again? What should be the criterion to open schools? Did any one of them – strong and very decisive politicians – even think about how to get out of this when they introduced it? And I think that would be a problem for the UK as well.
Q: So yes let’s take as a comparison your – the neighboring countries in Scandinavia. A lot of people are sending around these charts that show that Denmark and Norway and Finland have had much fewer deaths on a per capita basis and Sweden the rate is still climbing and they take that as proof essentially that Sweden should have gone into a more draconian lockdown. What do you say to those people?
A: Well first it’s not crooked Denmark. Secondly, one important thing is that Norway – the nursing homes in Norway are usually quite small. Whereas the nursing homes in Sweden are quite big, with hundreds of people. Which means that if you get in – if the virus gets in to one nursing home in Norway which will affect far fewer people than a big one. So that’s part of the reason, not all of the reason. For Finland the epidemic never really took up to cope there: they started their measures before it had even started. But I think we should have this discussion a year from now – let’s decide that on the 17th of April 2021. I think that the difference between countries would be quite small in the end.
Q: So that you don’t think that the severity of these intervening measures are gonna make that much difference?
A: No, I don’t think so. I think it – should I tell you what I really think? [Please.] I almost never do this. I think what we’re seeing is a tsunami of a usually quite mild disease which is sweeping over Europe – and some countries do this, and some countries do that, and some countries don’t do that – and in the end there was very little difference.
Q: So when you say it’s a usually quite mild disease, what do you mean by that?
A: That most people who get it will never even notice they were infected.
Q: So does that mean that you think the actual fatality rate of this disease is much lower than the numbers that have been talked about?
A: Much, much lower.
Q: So do you – have you made any speculations as to what sort of zone the real fatality rate might be in?
A: I think it would be like a severe influenza season, the same as, and which would be an order of 0.1 percent maybe.
Q: So that would suggest then, for a country like the UK that has already had its heading towards 20,000 deaths, that would suggest that millions – many millions – of people have already had it?
A: Yes.
Q: And you believe – do you think that is also true in Sweden then? That a substantial percentage of the population has had it?
A: Yep. I’m rather certain on that, actually.
(Link)
As the Covid-19 crisis progresses, censorship programs advance, amid calls for China-style control of the Internet:
The Inevitable Coronavirus Censorship Crisis is Here
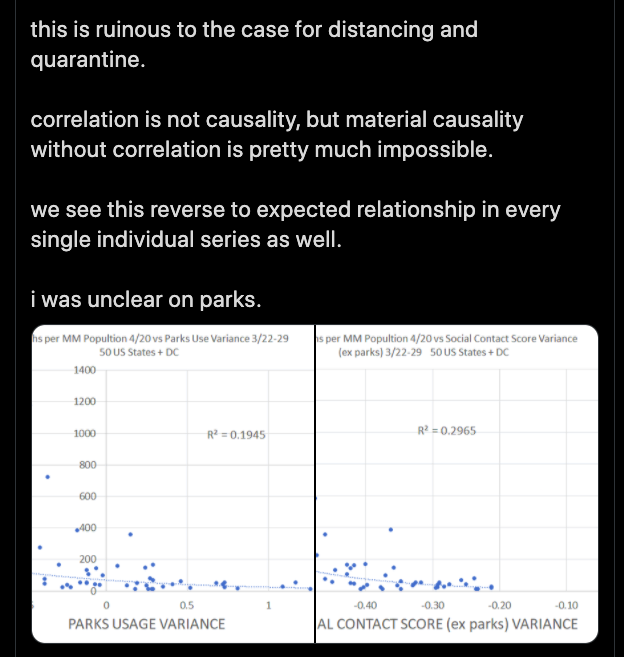
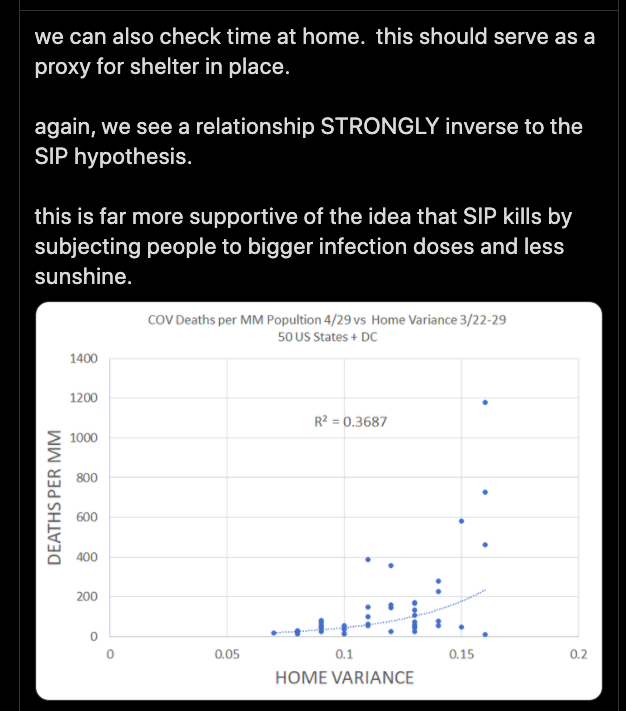
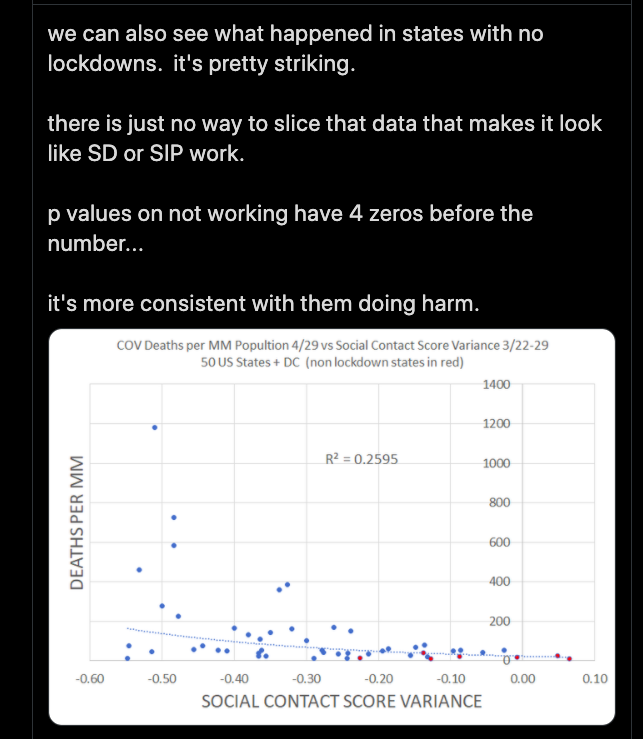
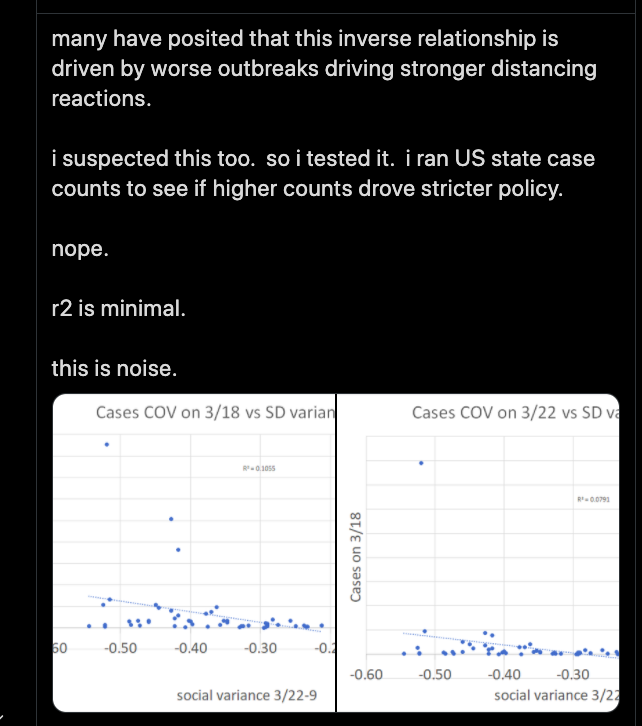
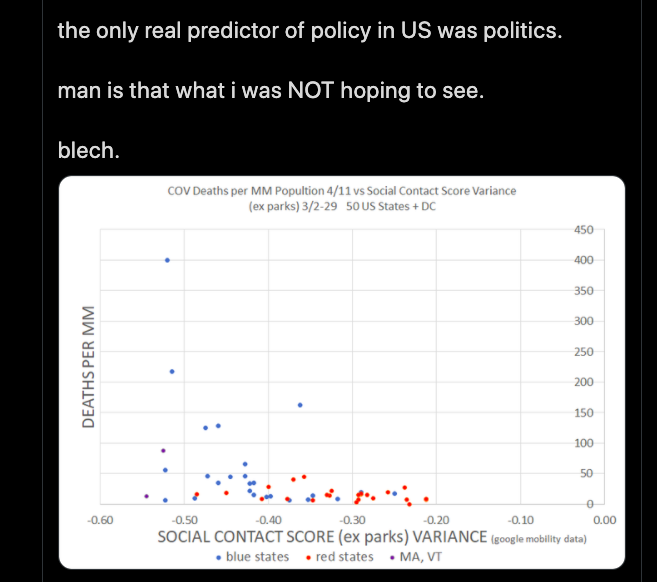
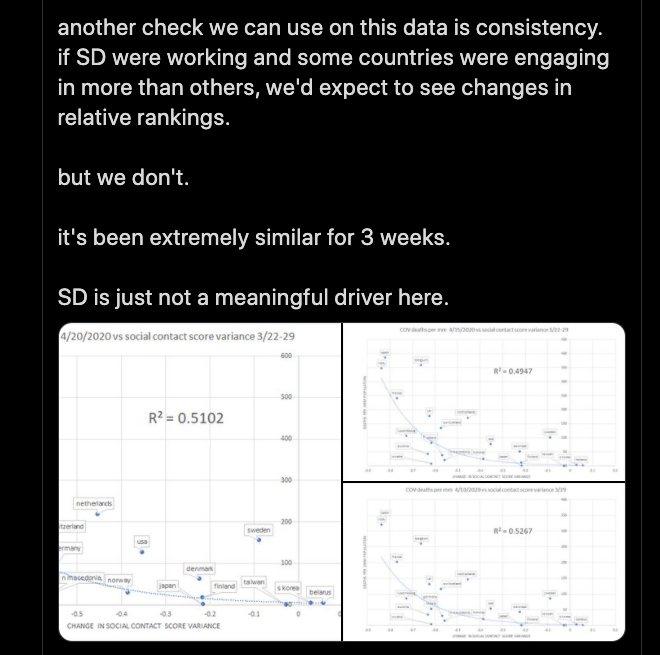
I close with the following data, compiled and painstaking plotted by el gato (statistician), and what you see below shows in no uncertain terms the mathematical truth about social distancing (SD, he abbreviates it) and the actual effects on death reduction. Please take a moment and process it:

Please consider what I have already said in previous posts. Please: the power which the state has seized by executive decree is a newfound power that’s unchecked, and even if you agree wholeheartedly with the motive and desired results of this particular power-play, remember the following and think about it carefully: it is an unjustly acquired state power over individuals and their property, yours included, and all your loved ones’ as well, and because it’s unchecked, it is a power that can now move in any direction, into any arena of human life, at any time.